I recently chatted with a VC invested in 15 healthcare apps that use Behavior Modification to facilitate patients through permanent behavior change for enhanced health. He said although many of his apps use it, there’s no scientific evidence that Behavior Modification works. Hmmmm… And the reason you’re still using it is… “There’s nothing else to use.”
I contend that current Behavior Mod approaches are not only faulty, but seriously harmful to a large population of people who need to consider permanent change. You see, Behavior Modification does NOT instigate new behaviors or permanently change existing ones. In diet, smoking cessation, and exercise maintenance alone, there is a 97% failure rate for ongoing adoption of altered behaviors.
Now let’s be honest here. If you’ve ever tried to keep lost weight off, or habituate a new exercise routine, or stop smoking, or… you’ve probably tried to modify your current behaviors by doing the same thing differently, or doing a different thing the same. Diets always work. It’s when we try to return to ‘normal’ that our lost weight returns. The problem isn’t the diet.
This essay is about conscious behavior change. For this, I must take you to the source – into your brain – to not only understand why you behave the way you do or resist new behaviors, but HOW to actually elicit the behaviors you want. Conventional thinking usually explains the WHAT and WHY, but fail to teach the HOW. In this article I’ll lead you through HOW your brain causes your behaviors, and where the inflexion points are so you can intervene and consciously design your own behaviors (or lead your patients and clients through to their best choices). I’ve tried to make the more procedural stuff fun and relatable so you’ll barely notice. Enjoy.
BEHAVIOR
There are two major problems with Behavior Modification:
1. Behavior 2. Modification.
I suspect most people haven’t considered what a ‘behavior’ denotes. Behaviors are our identity, our beliefs, our history/norms/life experience in action, in the service of representing us to the world, to show people through our actions what we stand for. It’s how we show up as ‘us’ every day – the demonstration, the expression, the translation of who we are – the external actions that portray our internal essence, beliefs, and morals. Like an autobiography is the written representation of a life but not THE life. Like going to church represents us practicing our faith but not FAITH. Behaviors are the visible depictions of each of us.
Behaviors don’t occur without a stimulus. Nor do they operate in a vacuum. And they are always, always congruent with our beliefs. You know, without asking, that someone wearing a bathing suit to a church wedding most likely has different beliefs than the other guests. It’s not about the bathing suit.
In our brains, behaviors are the output of physiological signals, much as words and meaning are the output of our brain’s interpretation of electrical signals coming into our ears. In other words, it’s all happening unconsciously through brain chemistry: behaviors are merely the end result of a very specific sequence of chemical signals in our brains that traverse a series of congruency checks that ultimately agree to act.
Below is a summary of the physiology of what happens in our brains – the step by step path – that ultimately leads to behaviors. Here you’ll recognize exactly where and why Behavior Mod fails. For those wanting to skip the brain stuff, go directly to the CASE STUDY below. But don’t forget to peek at the great graphic of the HOW of decision making just below.
THE PHYSIOLOGY OF BEHAVIOR
For those of you who love to learn esoteric stuff, here is an overview of the physiology of our brain’s path to a behavior: from an Input/Cue that starts the process and signals that an action is requested, through our filters and trials that check the signal for risk, through to a STOP or an Output/Behavior. It’s what our brain does to cause us to behave, or not.
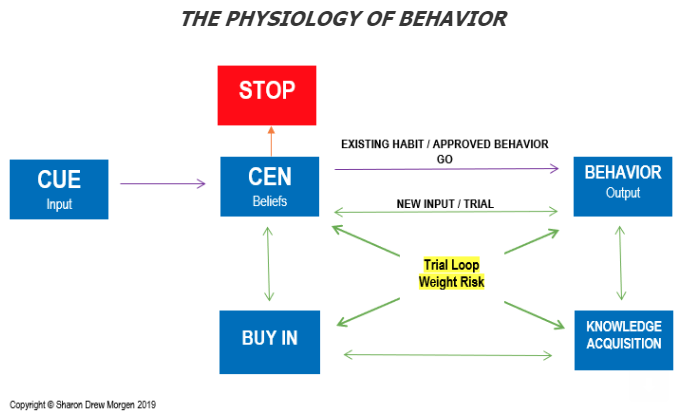
SIGNAL/CUE/MOTIVATION/INPUT: We start by giving ourselves some sort of CUE, an instruction or request, to take action, whether it’s to brush our teeth, or move our arm, or eat a salad. This signal traverses a neural pathway to get to the next stage, the CEN.
CEN/BELIEF FILTER: Our Central Executive Network, or CEN, filters all requests through our beliefs, morals, and norms. If the incoming cue is congruent with our beliefs and determined to have no risk, we peruse our lifelong history and trillions (literally) of neural pathways to find an existing behavior we’ve used before that matches the request. If one is found, there’s an immediate GO and you get a CUE –> BEHAVIOR, or in other words, INPUT –> OUTPUT match immediately. This happens when you get into your car and automatically put on your seatbelt, for example.
But if the motivating cue is incongruent with our norms and beliefs there is a STOP or resistance. This happens a lot when people try to do something they dislike, like add working out to their schedules, for example, because they believe they should – and they hate the gym, hate working out, and hate taking the time out of their day. Or something they’ve tried and have failed at. Or something that goes against their beliefs.
For the past 10 years, after decades of unsuccessfully trying to convince myself to get to the gym, I finally created a new habit and now go 8 hours a week – AND I HATE THE GYM. First I changed my cue. I told telling myself that as a healthy person, I believed (CEN) I am fit in mind, body, spirit. Now, if I want to be a slug, I ask myself if I want to be a healthy person today. Thankfully, I do 90% of the time.
The job of the CEN is to let in the good stuff and stop the bad. Behavior Mod doesn’t have the ability to change cues, and address belief filters.
TRIAL LOOP: If the CEN is congruent with the signal and there’s no behavior already in place, the signal goes into a trial loop where it
- assigns/weights/determines the risk of the new against the beliefs and norms (CEN);
- seeks new knowledge/learning tools to trial and practice behaviors that conform with the cue;
- while comparing against the filters in the CEN for congruence;
- develop a new neural pathway/synaptic connection for a new behavior if congruent (i.e. GO) or
- STOP a signal if a risk uncovered, and no new behavior is formed.
Obviously our brains are set up to filter out what they believe will harm us. And anything new that has not been bought into, or tested to fit in with our other norms, will be deemed a risk, regardless of the efficacy of the new or need for change.
When our cue gets stopped and doesn’t lead to a behavior it’s because
- We’re giving ourselves a cue that’s incongruent with who we are;
- We’re trying to use a pathway already developed for a different behavior;
- We’re attempting to change a behavior by starting from the output (behavior) end without going through the congruency process of weighting risk and getting Buy In.
Input (signal, cue, stimulus) –> CEN (beliefs) –> trial loop (congruency check) –> output (behavior)
You can see that behaviors are at the end of a chain of physiological events, the final step along the neural pathway between the input cue and action. The end. The response. The reaction. Nowhere do they occur on their own.
THE PROBLEM WITH MODIFICATION
Behavior Mod attempts to effect change at the output where an existing behavior is already in place, hoping that by practicing a preferred behavior over and over and over, different results will emerge. Obviously it can’t work. New behaviors activate and will permanently take hold ONLY once instructed by an input stimulus that has then been approved by your beliefs and weighted for risk and congruence.
In other words, when you try to change a behavior by trying to change an existing behavior, you’re trying to change the output without getting necessary Buy In for change. It’s not even logical. It’s why diets and exercise regimens fail: people try to change their existing habits rather than form wholly new ones with different signals that lead to wholly different – and more successful – routines.
Consider a robot that has been programmed to move forward but you want it to move backward. You tell it why ‘backward’ is best, you pitch it reasons it should want to move backward, you tell it a story about why moving backward is advantageous, and you even try to push it backward. But until you reprogram it, it will not go backward. It’s the same with us. We must create new incoming cues, go through a trial loop that weights risks/tries/fails/tries/fails, gathers necessary data along the way, and gets agreement to develop a wholly new neural pathway to a new action that’s congruent. You cannot change a behavior by changing a behavior.
It’s also impossible to expect permanent change when we omit the entire risk-check element of our Buy In process. The risk to our system of becoming imbalanced by shoving in something foreign into a system that’s been working just fine, is just too great, regardless of the efficacy of the new, and any new inputs will stop behaviors that haven’t been vetted. And Behavior Mod supersedes these tests by trying to push the change from the output end, before it’s been vetted.
HOW TO CHANGE BEHAVIORS PERMANENTLY
Here are three of the key elements involved in how we choose to behave differently. It’s systemic.
SYSTEMS CONGRUENCE. The role of systems here cannot be underestimated because they’re the glue that holds us together. I am a system. You are a system. Your family is a system. Every conglomeration of things that follow the same rules is a system. Every system has its own status quo – its own unique set of norms, beliefs, identifiers that show up, together, and are identified as Me, or My Family, or My Work Team. The system of people working together at Google will be different from the system of people working together at Kaiser Permanente, with unspoken rules that apply to dress codes, hiring practices, working hours, relationships, the way meetings are run.
The job of our status quo is to maintain Systems Congruence (You learned that in 6th grade. It means that all systems, all of us, seek balance, or Homeostasis.) so we can wake up every day being who we were yesterday. And all day, trillions of signals enter into our brains and lead us to behaviors that have met the criteria of systems congruence and safety. These are our habits. Indeed, our brains check all incoming signals for incongruence before behaviors are agreed to, making sure we remain in balance minutely.
Any time you try (and try and try and…) to behave in a way that unconsciously causes imbalance within you – when you push against an existing habit or action and try to get a different behavior – you’ll experience resistance or sabotage. For any proposed change, to maintain congruence, your system must agree, Buy In, in a way that matches your beliefs, identity, and norms. And it’s physiologic, chemical, automatic, and unconscious. Our brains do this for us every second of our lives. Behavior Modification supersedes this process, trying to induce behavior change in a way that risks generating imbalance, or Systems Incongruence – and inaction.
INPUT. Any new input signals will only become a behavior if they are congruent with the beliefs, identity and norms of the person’s system. When you wish to change a behavior, it’s necessary to input the correct message as all that follows is a response to the input cue. I recently asked a friend with a long history of trying to lose weight permanently what she tells herself to begin (her stimulus). ‘I tell myself I’m a disgusting slob.’ Since different inputs will be assessed by the CEN uniquely and each achieve different outputs, being a ‘disgusting slob’ will invite the same behaviors that caused her to be a ‘disgusting slob’ to begin with, and she’ll fail over and over; she’s inputting the same signal expecting a different response, but her brain will only seek/find the old response.
TRIAL LOOP. Because a new input seeking a new output/behavior demands a congruence test in the CEN to assess risk, there’s a trial process that includes
- adding new knowledge (education, books, coaching, lessons, etc.) to achieve new skills to trial;
- continual comparisons against the CEN, or against our beliefs and identity, as each iteration progresses, to test for congruence;
- Buy-In so our CEN, our beliefs and identity, concur with each iteration of trialing and failing as our brains go about weighting any risk;
- trialing any new behaviors for congruence, that result from adding the new knowledge.
If at any point a risk is determined to put the system out of congruence, it will stop the new behavior. If the input cue is determined safe, it will agree to create a new behavior. Not to kick a dead horse, but Behavior Mod does not address this at all. That’s why it fails so often.
So if my friend wanted to permanently lose weight, she’d input something like “I’m a healthy person”, discover which of her beliefs are connected to that (“As part of my health practice, I eat nutritionally healthful food that works well with my lifestyle.”), and go through a trial loop that would include her doing research and possibly blood tests to see what types of food best align with her being healthy, and end up with a new set of healthful eating behaviors. Ultimately she’d have a lifetime food plan that kept her healthy, congruent with her beliefs about herself and habituated into her life. And her eating would become part of her system and become habituated.
CASE STUDY
I’ll share a recent experience I had using this process with my neighbor. In it I’ll label each element within the Buy In process in the chart above.
My neighbor Maria once came to my house crying. Her doctor had told her she was borderline diabetic and needed to eat differently. He gave her a printed list of foods to eat and foods to avoid and sent her on her way. At my house she told me she’d been trying for months, lost some weight, but finally gave up and went back to her normal eating habits and gained back the weight. But she was fearful of dying from diabetes like her mother did. Apparently the fear of death wasn’t enough to change her eating habits. She asked if I could help, and I told her I’d lead her through to finding her own answers. Here was our exchange.
SDM: Who are you? [RESPONSE TO DOCTOR INPUT/CUE]
Maria: I’m a mother and grandmother. [CEN FILTER, IDENTITY]
SDM: What are your beliefs that go with being a mother and grandmother?
Maria: I believe I’m responsible for feeding my family in a way that makes them happy. [CEN FILTER, BELIEFS]
SDM: What is it you’re doing now that makes them happy? [CEN FILTER, IDENTITY]
Maria: I make 150 tortillas each morning and hand them out to all my children and grandchildren who come over on their way to work and school in the morning. They love my tortillas. But I know they’re bad for me with all the lard in them, even though I eat them. I’ve tried to stop, but since I’m making them for everyone, they are a big part of my diet. When the doctor told me I can’t eat them anymore, it felt like he asked me to not love my family. [NO BUY IN FROM CEN/STOP]
SDM: So I hear that tortillas are the way you keep your family happy but the lard in them is unhealthy for you. Is there any other way you can keep your family happy by feeding them without putting your own health at risk?
Maria: Hmmmm… I could make them corn tacos. They don’t have lard, and my family loves them. [TRIAL LOOP, BUY-IN]
Maria then invited her entire (huge) family for dinner and presented her daughter Sonia with her tortilla pan outfitted with a big red bow. [TRIAL LOOP, NEW BEHAVIOR] She told her family she couldn’t make tortillas any more due to health reasons, and proclaimed Sonia the new “Tortilla Tia”. She could, she said, make them corn tacos whenever they wanted and she would happily try out whatever they wanted so long as they were happy. [TRIAL LOOP, KNOWLEDGE ACQUISITION]
That simple switch in her food choices and her handover to Sonia helped her begin a healthy eating plan. It inspired her to research other food substitutions [TRIAL LOOP, KNOWLEDGE ACQUISITION] she could make to avoid having a chronic illness. Eventually, she lost weight and had a food plan more closely aligned with what her doc suggested. And of course, she could still make her family happy with her food and meet her beliefs. [NEW NEURAL PATHWAY, NEW BEHAVIOR]
As you can see, just from entering the problem with a different hat on – helping patients figure out their own route to change and Buy In instead of trying to drive it – using a different curiosity and a different questioning system, it’s quite possible to guide people to discover their own best choices that are congruent with who they are.
FACILITATE BUY IN THEN ADD BEHAVIOR MOD
I realize my ideas aren’t in the mainstream at the moment. But just because Behavior Mod has such a stronghold in the healthcare field doesn’t mean it can’t be reexamined or appended. And just because Behavior Mod has been the accepted model to induce change doesn’t mean it’s successful. Remember when we believed top down leadership was the way to go? Millions of books sold? Billions spent on consultants? I’m offering something new here that deserves consideration.
And it’s not either/or; it can be both/and. You don’t have to throw away what you’ve got, just add a front end to stimulate Buy In. I’ve used this approach to train a large number of sales folks globally to facilitate buying decisions and it was quite successful. And here’s an article I wrote on adding my change facilitation concepts to Behavior Mod, should you have interest.
There are plenty of uses for this add on. Think of enabling patient Buy In for obesity or cardio clinics, to help patients design a work-out regimen for heart health. Or for diabetes sufferers to design a healthful food plan for life. Or athletes trying to change an inferior swing, or develop a new pattern to their feet differently to run faster. What about helping yourself meditate daily or organizing your life. Or to get more sleep.
We can help people alter their behaviors in a way that’s not only congruent with who they are, but helps them make their own best choices. But not with Behavior Modification alone.
Contact me to put you on an advance list for a Buy In program I’m running in June with Learning Strategies. In it you’ll learn how to design your own flow chart from Cue to Behavior to have conscious choice whenever you want to make a change. And if you have any interest at all in testing this model, or just sharing ideas, I welcome the conversation. sharondrew@sharondrewmorgen.com.
______________
Sharon-Drew Morgen is a breakthrough innovator and original thinker, having developed new paradigms in sales (inventor Buying Facilitation®, listening/communication (What? Did you really say what I think I heard?), change management (The How of Change™), coaching, and leadership. She is the author of several books, including the NYTimes Business Bestseller Selling with Integrity and Dirty Little Secrets: why buyers can’t buy and sellers can’t sell). Sharon-Drew coaches and consults with companies seeking out of the box remedies for congruent, servant-leader-based change in leadership, healthcare, and sales. Her award-winning blog carries original articles with new thinking, weekly. www.sharondrewmorgen.com She can be reached at sharondrew@sharondrewmorgen.com.
9 thoughts on “Behavior Modification doesn’t modify behaviors: an essay on why it fails and what to use instead”
Pingback: Sharon-Drew Morgen » The Cost of Perceived Wisdom: how normalized thinking restricts Search and exposes us
Pingback: Sharon-Drew Morgen » Feedback: a route to collaboration and excellence
Pingback: Feedback: a route to collaboration and excellence | | Best Practice In Sales and Marketing
Pingback: The HOW of Change | What? Did You Really Say What I Think I Heard?
Pingback: You Can't Change a Behavior by Trying to Change a Behavior | Sharon-Drew Morgen
Pingback: The Cost of Perceived Wisdom: how normalized thinking restricts Search and exposes us - Sharon-Drew
Pingback: The HOW of Change™: the physiology of transformation - Sharon-Drew
Pingback: You Can’t Change a Behavior by Trying to Change a Behavior - Sharon-Drew
Pingback: Feedback: a route to collaboration and excellence - Sharon-Drew